Part 5 The Rossi Family
5.3 Rossi family case study 2: John Rossi – Myocardial infarction, coronary artery bypass grafting (CABG) surgery
Dima Nasrawi and Donna Wilson
Introduction to case study






 Learning Objectives
Learning Objectives
By the end of this case study, you should be able to:
- Identify associated risk factors with the development of chronic cardiac disease.
- Identify the impact of acute coronary disease.
- Discuss required lifestyle modifications for patients living with acute coronary disease.
- Identify required self-management strategies to manage acute coronary disease.
- Discuss the role of the nurse managing patients following cardiac surgery.
Scenario
John is a 47-year-old man, whose wife died 5 years ago. Recently he has been experiencing signs of health deterioration, including high blood pressure, cold sweats and radiating chest pain to his left arm. John has kept these signs and symptoms confidential, not sharing his health issues with the family. His signs are exacerbated by continual stress, anxiety, unresolved grief and the pressures of looking after his family’s farm. He recently restarted smoking, as a coping mechanism against the stresses that he has in his life. At a recent community event, with people gathering in a well-known tavern to celebrate Easter Sunday after a church mass, John experiences an episode of shortness of breath and crushing sensations of chest pain. His cousin Alberto rushes John to the emergency department of the nearest hospital (Lismore base). Upon arrival at the hospital, the emergency doctor sees on the electrocardiogram tracing that John has developed an elevated ST myocardial infraction, which requires emergency coronary artery bypass grafting surgery (CABGX4).
The family becomes really concerned about John’s diagnosis, especially as they have always known him as a healthy, active man. John is transferred to a large tertiary hospital in Queensland so he can have his surgery within 24 hours. This news is very difficult and scary for Elisabeth. She is extremely concerned about her dad undergoing a complex surgery and very frightened about losing her father. Elisabeth starts to show signs of extreme anxiety, especially as she lost her mother at a young age. Maria, Maximo and Elisabeth decide to move to a hotel nearby so they can visit John and support him during his recovery from a complex surgery.
After his surgery John is transferred to the intensive care unit (ICU) for 48 hours. During his stay in the ICU, John struggles with his breathing due to his history of smoking. The healthcare team supports John to use an incentive spirometer and try some deep breathing exercises. He also requires a high flow of oxygen (45 litres at 45% of oxygen). During his stay at the hospital, John also experiences high levels of blood glucose. An ongoing diagnosis of coronary heart disease makes him very anxious about his surgical wound and recovery after discharge.
During visits by Elisabeth, Maria and Maximo in the post-operative phase, the family is concerned to see John connected to such an array of monitoring devices, which includes telemetry, drains, intra dwelling catheter, intra venous canula and isolated wires. The nursing and inpatient cardiac rehabilitation teams play an integral part in reassuring John and the family about discharge arrangements. On John’s last day at the hospital, he is referred to an outpatient cardiac rehabilitation program and provided with 2 follow-up appointments with cardiac surgeons and the outpatient department.
 Thinking points
Thinking points
Cardiac rehabilitation history, inpatient, outpatient, long term:
The management of myocardial infarction (MI) has changed significantly since 1950. However, cardiac rehabilitation (CR) remains underutilised treatment. The figure below shows the history of CR:
Figure 1:
History of cardiac rehabilitation
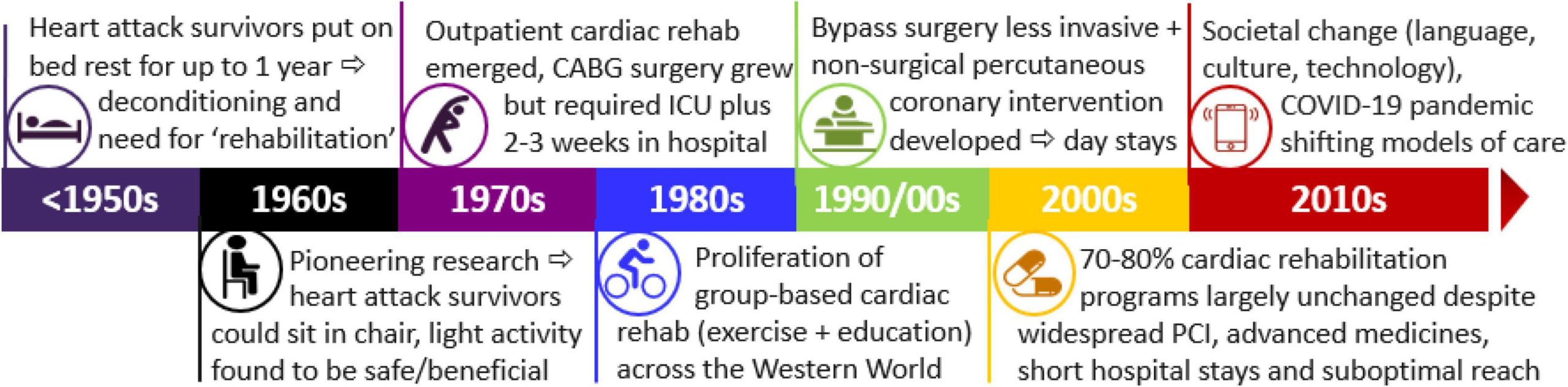
Now patients who survive an MI not only require a reperfusion similar to what John has undergone, but also an inpatient cardiac rehabilitation intervention that starts pre-operatively, continues after surgery and then after discharge (Nasrawi et al. 2022).
- Phase 1 cardiac rehabilitation focuses on introducing mobilisation to patients and required information for discharge and recovery.
- Phase 2 is an outpatient hospital-based program that includes a group and runs for 6 to 12 weeks.
- Phase 3 is known as the maintenance phase and is usually around 4 to 6 months where patients learn how to continue their exercise regime, risk factor modification and return to work and their daily lifestyle.
Thinking point
In Australia, 12,700 CABG procedures were performed between 2020 and 2021 (Australian Institute of Health and Welfare [AIHW], 2023.) Surgical intervention can lead to various adverse events, with hospital-acquired infections being the most common complications. Including patients in healthcare improvement is paramount and is supported by the Australian national safety and quality health service standards. This approach includes a collaboration between practitioners and the patient, the use of photographs to allow accurate evaluation and documentation of the wound healing process.
 Case study questions
Case study questions
- What local organisations support recovery after heart surgery?
- Who in the interdisciplinary team cares for a patient during the inpatient cardiac rehabilitation phase after cardiac surgery?
- Who in the interdisciplinary team cares for a patient during the outpatient cardiac rehabilitation phase after cardiac surgery?
- What are the 3 phases of cardiac rehabilitation?
- What is the impact of diabetes on wound care after surgery?
- How do you provide culturally sensitive care for patients after cardiac surgery? (refer to the Shero family in Part 3 for additional information about cultural sensitivity)
Key information and links to other resources
- Heart Foundation: What is coronary heart disease?
- Heart Foundation: Find a cardiac rehabilitation service near you
- Diabetes Australia
What is a myocardial infarction?
John experiences a feeling of crushing chest pain or in medical terms an ‘unstable angina’. His angina is associated with atherosclerosis plaque, thrombus and was not relieved by rest. The occlusion escalates to an ST-elevation myocardial infarction.
Symptoms of a myocardial infarction, or ‘heart attack’ can be different for each person, ranging from serious to mild. The most commons symptoms include:
- Pain or tightness in one of these areas: chest, arms, shoulders, neck or jaw.
- Shortness of breath, feeling dizzy, sweaty or nausea.
For example, this flyer should be available in every household, especially in John’s house, to detect early signs and trigger an early response. The Heart Foundation website has many resources that can assist patients and families to manage coronary artery disease, including videos and flyers in various languages:
 Case study 2 summary
Case study 2 summary
John’s case covers the importance of early detection of signs of myocardial infarction and early management to improve health outcomes. While reperfusion therapy is vital to increasing chances of survival, cardiac rehabilitation, or, in more inclusive terms, secondary prevention, is essential to implementing lifelong preventative strategies.
References
Australian Institute of Health and Welfare. (2023). Heart, stroke and vascular disease: Australian facts. https://www.aihw.gov.au/reports/cvd/092/hsvd-facts/contents/treatment-and-management/hospital-care-and-procedures
Nasrawi, D., Latimer, S., Massey, D., & Gillespie, B. M. (2023). Delivery, barriers, and enablers to patient participation in inpatient cardiac rehabilitation following cardiac surgery: An integrative review. Australian Critical Care, 36(3), 420–430. https://doi.org/10.1016/j.aucc.2022.01.007
Redfern, J., Gallagher, R., O’Neil, A., Grace, S. L., Bauman, A., Jennings, G., Brieger, D., & Briffa, T. (2022). Historical context of cardiac rehabilitation: Learning from the past to move to the future. Frontiers in Cardiovascular Medicine, 9, Article 842567. https://doi.org/10.3389/fcvm.2022.842567
Suggested readings
Walker, R., Lin, F., Chaboyer, W., Latimer, S., Eskes, A., Clayton, C., Murphy, C., Sladdin, I., Bull, C., & Gillespie, B. (2020). Identifying surgical wound care priorities from the perspectives of clinicians and health consumers in an Australian private healthcare context: A case study. Wound Practice & Research, 28(1), 17–21. https://doi.org/10.33235/wpr.28.1.17-21
