Imaging tests
Payne Stark
Chest x-ray - handout available
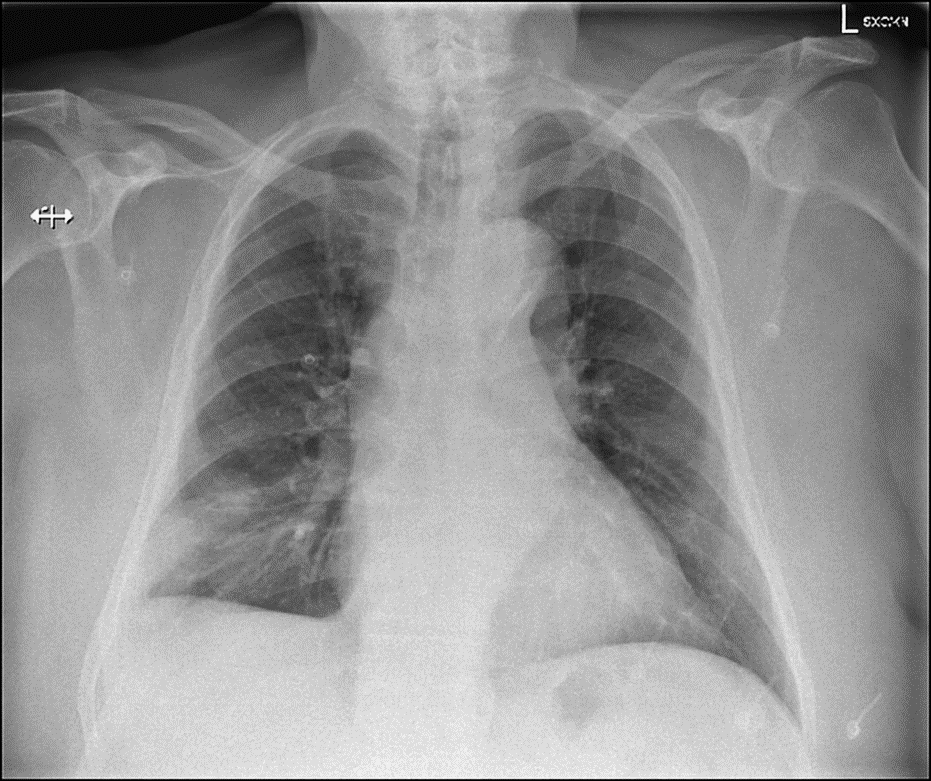
Interpretation. Do not provide to student/team unless requested in consultation.
Enlarged cardiac silhouette. Hilar regions are unremarkable. Focal area of air space opacification within the peripheral right lower zone, obscuring the right costophrenic angle. No pneumothorax. No acute bony or soft tissue changes. Appearance compatible with infection, haemorrhage or pulmonary infarction due to pulmonary embolism.
CT Pulmonary Angiogram – handout available
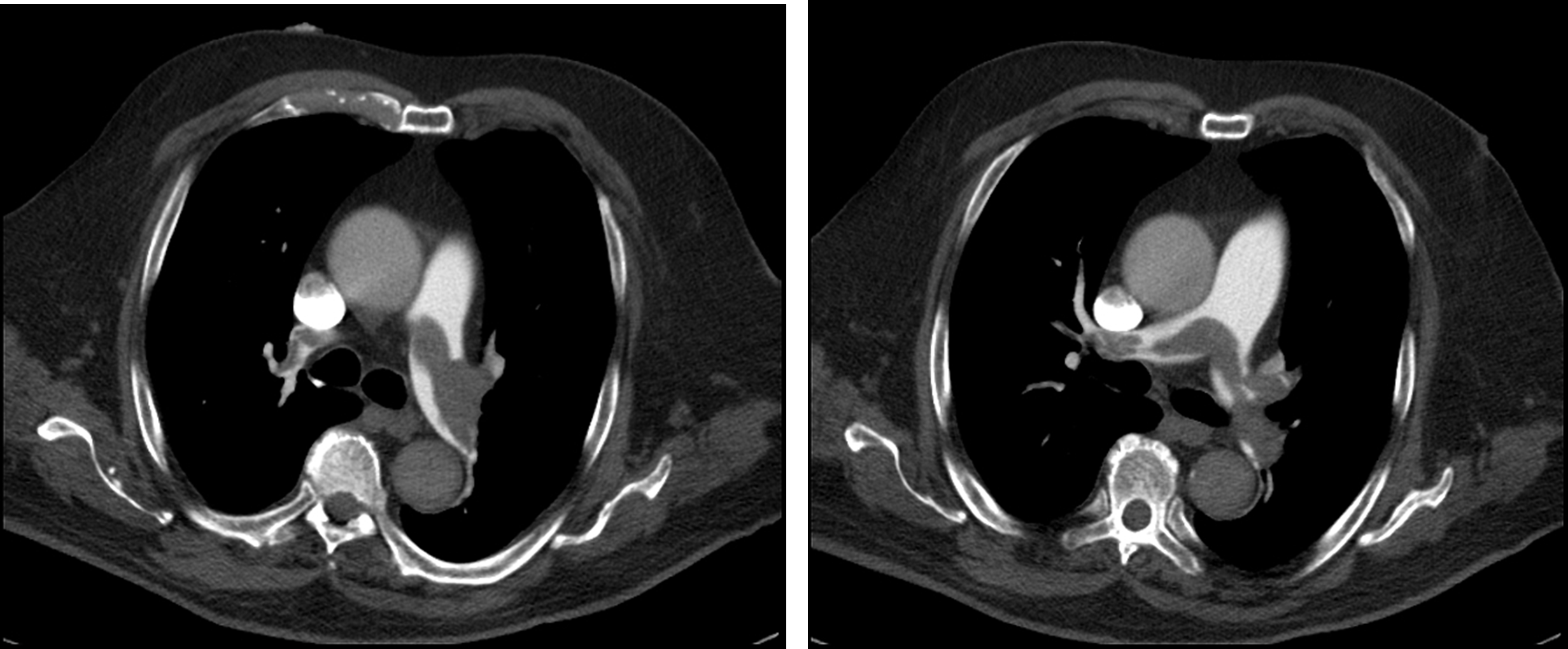
Interpretation: Large saddle pulmonary embolism with associated RLL pulmonary infarcts and evidence of right heart strain. Complete interpretation provided in student/team handout.
Other imaging
| Investigation | Case result |
|---|---|
| Barium Enema | Normal |
| Barium Swallow | Normal |
| CT Abdomen/Pelvis | Normal |
| CT Chest (High Resolution) | Radiologist recommends CT Pulmonary Angiogram instead – upgrade at no cost |
| CT Coronary Angiogram | Unsuitable to perform |
| CT Head | Normal |
| CT KUB (Kidneys, Ureters, Bladder) | Normal |
| CT Pulmonary Angiogram | See above |
| Echocardiogram | Normal LV size and systolic function. RV appears dilated with impaired function. |
| Mammogram | Normal |
| MRI (General) | Normal |
| MRI Brain | Normal |
| Nuclear Medicine / Ventilation Perfusion scan | Significant perfusion defects with normal ventilation, consistent with the diagnosis of pulmonary embolism. |
| Ultrasound Scan | Left leg venous doppler US study shows two of the three lower leg veins and the popliteal vein are filled with an echogenic non-compressible thrombus. |
| X-Ray Abdomen | Normal |
| X-Ray Chest | See above |
| X-Ray Orthopaedic (Hands/Knees/Bone Age) | Normal |
