Prematurity and deviations from fetal growth
Key Concepts
- Prematurity
- Small for gestational age infant
Preterm birth is significant due to the complications that arise from prematurity which can affect the infant’s survival and later development. These complications stem from immature organ systems that are not yet equipped to function outside the womb. As gestational age increases, the risk of acute neonatal illness decreases, highlighting the vulnerability of the brain, lungs, immune system, kidneys, skin, eyes, and gastrointestinal system. Preterm infants are at a higher risk of neonatal mortality (within the first 28 days) compared to those born full term, with mortality rates rising as gestational age or birth weight decreases (Behram and Butler 2007).
Terminologies
- Premature infant: infants born less than 37 weeks
- Late preterm infant: 34 – 36.6 weeks
- Moderate preterm infant: 32 -33.6 weeks
- Very preterm infant 28 -31.6 weeks
- Extreme preterm infant less that 28 weeks
- Fetal growth restriction: <10% centile + Doppler indices of placental dysfunction- Fetal growth restriction (FGR) describes the fetus that does not grow to its expected biological potential in utero and is a relatively common complication of pregnancy.
- Small for gestational age (SGA): < 10th centile for population, 50 – 70% constitutionally small including weight & abdominal circumference
- Average for gestational age (AGA)- those between the 10th and 90th percentiles
- Large for gestational age (LGA): >90th centile, 10% higher weight-for-age ratio than their counterparts
- Low birth weight (LBW): < 2500g
- Very Low birth weight (VLBW): <1500g
- Extremely LBW: <1000g
(Balest 2025, Kain and Mannix 2023)
Physical characteristics of the premature infant
Premature infants (those born before 37 weeks of gestation) can face a variety of complications related to the immaturity of their organs and systems. The severity of these complications depends on how early the infant is born. Here are some the distinguishing physical features of prematurity as well as some of the more commonly seen complications of prematurity and structural characteristics associated with these.
Some of the physical characteristics of a premature infant may include but not limited to the following:
-
- Skin: less than 27 weeks very thin and translucent, may look red. The epidermis of a preterm infant has fewer cell layers, which makes it more susceptible to injury and heat loss, and it has increased permeability. The stratum corneum layer of the epidermis begins to develop at 15 weeks’ gestation, however the formation of a functional barrier is not present until around 34 weeks’ gestation.
- Lanugo: the fine downy hair over the body develops between 16-20 weeks’ gestation and often sheds between 29-40 weeks’ gestation, however certain ethnicities may have a more abundance of lanugo than others.
- Plantar Creases: at 28 weeks the sole of the foot is generally flat with a single crease, at 32 weeks deepen creases on the sole of the foot which extends throughout gestation
- Breast tissue: in very preterm infants at 28 weeks no breast tissue nipple is barely visible and the areola non-existent. By 34 weeks breast nodule is palpable
- Ear cartilage: up until 32 weeks there is little cartilage the ear retains the shape applied to it. By term the ear is fully shaped and recoils immediately after deformation.
- Genitalia: The female labia minora and clitoris are prominent in early gestation. By term the labia majora have developed and cover the labia minora and clitoris. In the male the testes descend into the scrotum at 29 weeks’ gestation, but may not be deep within the scrotum until term
- Eyelids: may remain fused until 25 weeks’ gestation
(Balest, 2025, Furdon 2023 Gardner et al 2021, Kain and Mannix 2023)

Premature infant with ventilator by ceejayoz from Wikimedia Commons is licenced CC BY 2.0
Neurological complications
An underdeveloped neurological system, immature brain development, which is highly vascular and more susceptible to bleeds due to fragile vessels which are more susceptible to rupture. The premature infants’ neurological system lack of myelination and has a reduced ability to regulate fluctuations in blood flow to the brain (hypotension/hypertension), as well as being more susceptible to infection such as meningitis.
Complications include but not limited to:
-
- Intraventricular Haemorrhage (IVH): Bleeding in the ventricles of the brain due to the immaturity of their cerebral vasculature and poor regulation of cerebral blood flow, this is more common in extremely premature infants, with severe IVH leading to long-term developmental problems
- Periventricular Leukomalacia (PVL): Damage to the brain’s white matter due to lack of blood flow causing ischemia and or inflammation, often associated with premature birth, which can lead to motor and cognitive delays
- Neurodevelopmental Delays: Premature infants are at higher risk for developmental delays related to the above two causes. Developmental delays may include learning disabilities and problems with motor skills and coordination.
- Apnoea of Prematurity is the temporary cessation of breathing for greater than 20 seconds due to immature respiratory control mechanisms, greater risk of developing apnoeic episodes less that 34 weeks
(Blast 2025, Furdon 2023, Gardner et al 2021, Kain and Mannix 2023).
Respiratory complications
An underdeveloped respiratory system, due to immature lung structures, poorly developed alveolar saccules, inadequate pulmonary capillary bed as well as surfactant deficiency leads to “stiff” (non-compliant) lungs.
Surfactant starts being produced around 24 weeks (canalicular stage) with surge around 34 weeks (saccular stage). This is coupled with an immature respiratory control centre, high chest wall compliance / weak respiratory muscles, narrow nasal airway, as well as being obligatory nose breathers (all infants have no compensatory mechanism if nasal obstruction), and a poor cough/gag reflex.
Complications include but not limited to:
-
- Respiratory Distress Syndrome (RDS): due to the lack of pulmonary surfactant which starts being produced around 24-28 weeks’ gestation with a surge around 32-34 weeks’, generally by 35 weeks’ gestation the fetus should have sufficient levels to support independent breathing. The extreme preterm infant also has limited and or immature alveoli, these continue to grow and develop right through to the alveolar stage of lung development between 36 weeks to 3+ years postnatal age.
- Apnoea of Prematurity: due to immature respiratory control mechanisms, and respiratory muscle fatigue, greater risk of developing apnoeic episodes less that 34 weeks
- Bronchopulmonary Dysplasia (BPD): A chronic lung disease that can develop in premature infants, especially those who needed prolonged ventilation or oxygen support.
- Transient Tachypnoea of the Newborn (TTN): A temporary condition causing rapid breathing due to delayed clearance of fetal lung fluid
(Blast 2025, Furdon 2023, Gardner et al 2021, Kain and Mannix 2023).
Cardiovascular complications
An underdeveloped cardiovascular system and immature contractile tissue within the ductus arteriosus, leads to less sensitivity to increasing circulation oxygen and increased sensitivity to dilating effects of circulating maternal prostaglandins. This is coupled with a decreased circulating blood volume, limited ability to vasoconstrict blood vessels and adrenal insufficiency.
Complications include but not limited to:
-
- Patent Ductus Arteriosus (PDA): A persistent opening of the fetal shunt between the pulmonary artery and the aorta that can lead to abnormal blood flow, potentially requiring medical or surgical intervention.
- Hypotension: Premature infants may have low blood pressure due to underdeveloped circulatory systems.
(Blast 2025, Furdon 2023, Gardner et al 2021, Kain and Mannix 2023).
Gastrointestinal complications
Premature infants are at risk due to an underdeveloped gastrointestinal system and an immature glucose response, as well as an undeveloped suck, swallow, breathe reflex which starts developing at approximately 34 weeks’ gestation, and a poor gag and cough reflexes. These immature systems can lead to incompetent cardiac sphincter, incompetent ileocecal valve and impaired recto-sphincteric reflex which may increase the risk of necrotising enterocolitis (NEC). This coupled with delayed gastric emptying, small stomach capacity, decreased intestinal motility putting them at increased risk of enteral feed intolerance. Low glycogen stores in liver and fat stores increases the risks of hypoglycaemia and hypothermia (Blast 2025, Furdon 2023, Gardner et al 2021, Kain and Mannix 2023).
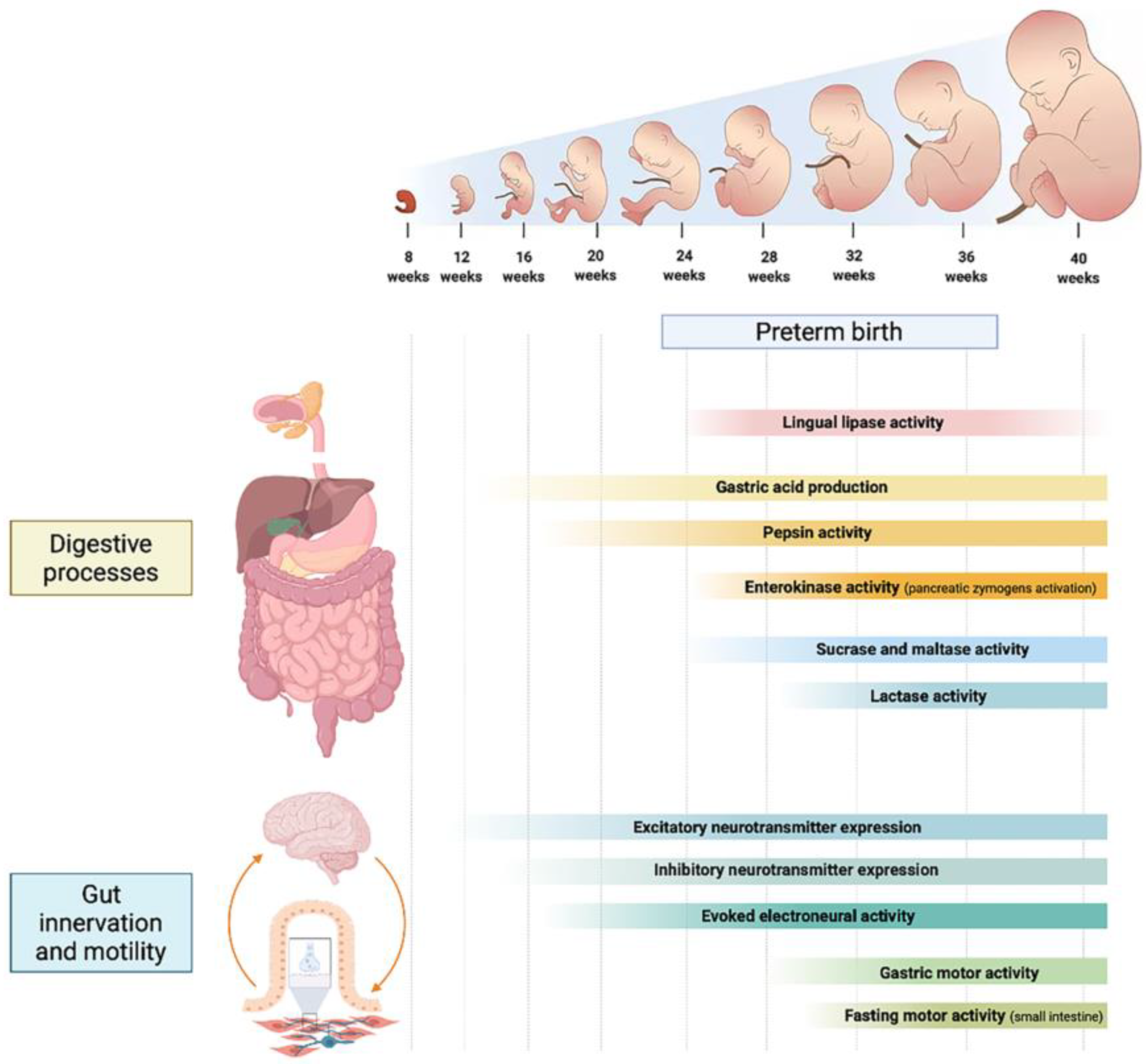
Image Attribution and Text description
Image Figure 1 from Indrio F, Neu J, Pettoello-Mantovani M, Marchese F, Martini S, Salatto A, Aceti A. Development of the Gastrointestinal Tract in Newborns as a Challenge for an Appropriate Nutrition: A Narrative Review. Nutrients. 2022; 14(7):1405. https://doi.org/10.3390/nu14071405 licenced CC BY 4.0
Image description: Image depict the development of the digestive processes and the gut in utero. Development starts from weeks 12 – 16 and continues through to birth.
End of Attribution and Description
Gastrointestinal complications include but not limited to:
-
- Poor feeding: Premature infants may struggle with oral feeding due to underdeveloped oral-motor skills (suck swallow breathe coordination believe to start developing around 32-34 weeks’ gestation), this can lead to difficulties in breastfeeding or bottle-feeding with increased risks of aspiration, apnoea and or desaturations. Parents and care givers are encouraged to look signs of feeding readiness (feeding cues rooting reflex, bringing hand to mouth, sucking on hands, fingers or pacifier, a quiet alert state, an increase in activity when a feed is due)
- Feeding intolerance: due to immature gut motility and delayed gastric emptying accompanied with underdeveloped digestive enzymes (lactase, lipase and amylase). Some premature infants may also have altered gut microbiome. Feeding intolerance may also be caused by too early or rapid advancement of enteral feeds which can overwhelm the immature GI system.
- Hypoglycaemia: Premature infants have limited glycogen stores, immature liver function, inadequate fat stores and a higher glucose demand placing them at higher risk of hypoglycaemia (Blood glucose level less than 2.6 mmol/L). This risk is increased if feeding is delayed or insufficient.
- Growth Restriction: Premature infants may not grow as quickly as full-term infants and may require more careful nutritional support.
- Necrotising Enterocolitis (NEC): due to immature gut mucosal barrier it is a life-threatening intestinal disease more common in premature infants, causing inflammation and bacterial infection of the intestines, which may lead to perforation or bowel necrosis.
- Gastroesophageal Reflux (GOR): Premature infants may have difficulty with proper digestion, leading to reflux and vomiting
(Blast 2025, Furdon 2023, Gardner et al 2021, Kain and Mannix 2023).
Immune system complications
An underdeveloped immune system, lower levels of immunoglobulins transferred in later pregnancy, immature gastrointestinal system and an immature Integumentary system, thin stratum corneum -more permeable. Fewer fibrils connect dermis to epidermis equals greater risk of abrasion/friction injuries (Furdon 2023 Gardner et al 2021, Kain and Mannix 2023).
Complications include but not limited to:
-
- Infection related to an immature immune system: Passive immunity from maternal antibodies increases substantially during the third trimester, infants are born before 32 weeks (or the third trimester) do not have the benefits of these antibodies in their system which increases their susceptibility to infections such as sepsis, respiratory infections, and urinary tract infections
- Increased Risk of Hospital-acquired Infections: Premature infants are often admitted to the neonatal unit for an extended period and receive multiple invasive procedures; for example, insertion of intravenous lines, blood sampling, feeding tube insertion, suctioning and intubation, which increases their risk of acquiring hospital borne infections
Thermoregulatory complications
An underdeveloped thermal control response, large surface area to body mass ratio, extended posture – limited ability to assume flexed position, decreased physiological flexion: Total body muscle tone is reflected in the infant’s preferred posture at rest and resistance to stretching of individual muscle groups. As maturation progresses, the fetus gradually assumes increasing passive flexor tone that proceeds in a centripetal direction, with lower extremities slightly ahead of upper extremities. Thin, permeable skin and unable to shiver, or sweat (Poor function of sweat glands). This coupled with hypoxia or hypoglycaemia preventing infants from generating adequate heat through metabolism (due to limited glycogen stores, low brown fat stores and low subcutaneous fat stores, delayed ability to initiate gluconeogenesis and poor respiratory function).
Complications include but not limited to:
-
- Hypothermia (low body temperature less than 36.5o C), especially in the first days after birth due to large surface area to body mass ratio, limited brown fat, limited subcutaneous fat and thin skin
- Hyperthermia (high body temperature greater than 37.5o C),
- Hypoxemia (PaO2 less than 40 mmHg) and Hypoglycaemia (blood sugar less than 2.6 mmol/L)- secondary to hypothermia due to increased metabolic demands in an attempt to create heat

(Blast 2025, Furdon 2023, Gardner et al 2021, Kain and Mannix 2023).
Other conditions associated with prematurity
Vision Problems- Retinopathy of Prematurity (ROP): Abnormal growth of blood vessels in the retina, which can lead to vision problems or blindness, particularly in infants born before 32 weeks of gestation. Exposure to excessive oxygen supresses vascular endothelial growth factor which halts normal vessel growth
Hearing Impairment Premature due to immaturity of the cochlea and auditory brainstem pathways infants are at a higher risk for hearing loss, especially if they require prolonged exposure to loud noises (e.g., ventilators, slamming of incubator doors) or receive ototoxic medications
Long-term Developmental Issues Premature infants may experience ongoing developmental challenges, including speech and language delays, motor skill delays, and social-emotional issues. Early intervention programs can help mitigate these effects.
Impaired Kidney Function Premature infants are more likely to experience issues related to kidney function, including acute kidney injury and difficulty maintaining electrolyte balance.
(Blast 2025, Furdon 2023, Gardner et al 2021, Kain and Mannix 2023).
Low birth weight (LBW) infants are considered less than 2500grams at birth. Although, it is important to distinguish between the ‘healthy but small’ as opposed to the ‘unwell, growth restricted’ infant. The causes for being small are varied, but more commonly due to prematurity, genetically small and fetal growth restriction. Whether prem or small for gestational age (SGA), an interruption has occurred in-utero that prevents the optimal environment for normal physiological and neurodevelopmental growth. This alone can impede development and growth. “Being born small lays the foundation for short-term and long-term implications for life ” (Malhotra et al. 2019). Implications of being born small include the inability to self-regulate due to immature regulatory and central nervous system, infant no longer has the protection of uterine environment & amniotic fluid to provide that postural containment, establishing breastfeeding is challenging, and failure to meet growth trajectory expectations.
Causes of reduced growth can be divided into 4 main categories:
- Maternal: malnourished, hypertension, pre-eclampsia, renal disease, illicit drugs
- Fetal: chromosomal abnormalities, multiple fetuses (limited placenta for multiple fetuses), congenital infection (cytomegaly virus, rubella, syphilis, toxoplasmosis), congenital malformations, congenital heart disease, diaphragmatic hernia, trachea-oesophageal fistula
- Placental factors: dysfunction or insufficiency, infarction, placental separation, twin-twin transfusion.
- Constitutional and ethnicity small.
Fetal growth restriction (FGR)
Fetal growth restriction (FGR) refers to a fetus that does not achieve its expected growth potential in utero and is a common pregnancy complication. Unlike constitutional smallness, true FGR is a pathological condition caused by placental insufficiency, where the placenta does not provide enough oxygen and nutrients to the developing fetus. An infant is considered FGA if their weight is below the 10th percentile for their gestational age. This means they are smaller than 90% of infants at the same gestational age (Malhortra et al 2019).
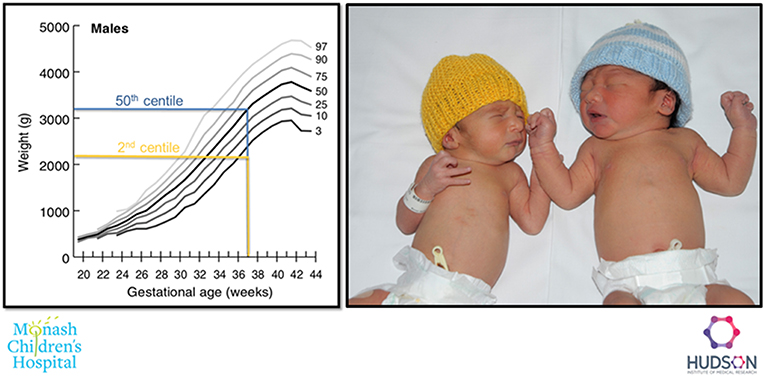
Example of a FGR (2nd centile weight for age, yellow), and an appropriately grown (50th centile weight for age, blue) both infants born at 37 weeks’ gestation, Figure 2 in Neonatal Morbidities of Fetal Growth Restriction: Pathophysiology and Impact by Malhotra, Allison, Castillo-Melendez, Jenkin, Polglase and Miller is licenced CC BY 4.0
There are two types of FGR, these are summarised below:
| Symmetrical FGR | Asymmetrical FGR | |
| Definition | The entire body of the fetus is proportionately smaller. This means that both the head and the body are reduced in size. | The fetus has a normal-sized head but a smaller body, leading to a disproportionate appearance. |
| Causes | This type is often associated with conditions that affect the fetus early in pregnancy, such as genetic disorders, congenital anomalies, or maternal factors (e.g., chronic health issues, poor nutrition). | This type usually occurs later in pregnancy and is often associated with placental insufficiency or other issues that affect nutrient and oxygen supply. It can result from maternal factors like high blood pressure or diabetes. |
| Characteristics | Infants with symmetrical IUGR tend to have a more uniform decrease in size across all body parts, brain growth not preserved | Infants with asymmetrical IUGR may have a larger head relative to their body size, as the brain prioritises growth when resources are limited (‘brain sparing’) |
| Outcomes | High risk of perinatal mortality. High risk of neurological impairment due to impaired brain growth. Catch up growth limited | Moderate risk of perinatal mortality. Lower risk of neurological impairment due ‘brain-sparing’. Catch up growth often good in both head and body size |
(Gardner et al 2021, Kain and Mannix 2023, Malhortra et al 2019).
In summary
Being born prematurely can impact the neonate’s survival and future development, complications are mainly due to underdeveloped organ systems that are not fully equipped to function independently outside of the uterus.
Birthweight that reflects intrauterine growth restriction is an important determinant for perinatal morbidity and death and, in recent years, has been shown to be a marker of postnatal life-course health risks. “Being born small lays the foundation for short-term and long-term implications for life “(Malhotra et al. 2019)
Test your understanding
References
Balest, A. (2025 Preterm infants. MSD manual-Professional version. https://www.msdmanuals.com/professional/pediatrics/perinatal-problems/preterm-infants
Behram. R. and Butler. A. (2007) Preterm birth, causes, consequences and prevention. Institute of medicine. The national academies press. https://www.ncbi.nlm.nih.gov/books/NBK11385/
Fulton, S. (2023) Prematurity Differential Diagnoses. Medscape. https://emedicine.medscape.com/article/975909-differential?form=fpf
Gardner, S., Carter, B., Enzman-Hines, M. and Niermeyer, S. (2021) Merenstein and Gardner’s Handbook of Neonatal Intensive Care. 9th Edition. Elsevier.
Kain, V., and Mannix, T. (2023). Neonatal Care for Nurses and Midwives. Principles for Practice. 2nd Edition. Elsevier.
Malhortra. A., Allison. B., Castillo-Melendez. M., Jenkin. G., Polglase. G., and Miller. S. (2019) Neonatal Morbidities of Fetal Growth Restriction: Pathophysiology and Impact. Frontiers in Endocrinology vol 10 https://doi.org/10.3389/fendo.2019.00055
Fetal growth restriction
Intrauterine growth restriction

{kind=link}